Idaho abortion patients traveling to WA increased more than 50 percent after Dobbs

By Lauren Gallup and Rachel Sun
The big shift
(Runtime 1:34)
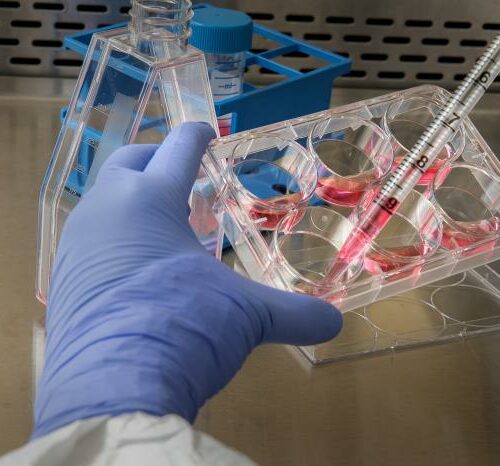
One year after the Supreme Court ruled to overturn the constitutional right to abortion, Washington Planned Parenthood clinics saw a 56% increase in Idaho abortion patients.
The data from Planned Parenthood, compiled by Senator Maria Cantwell’s office compares patient data from January to May of 2022 and the same months in 2023. It also showed out-of-state abortion patients increased by 36%, with an 18% increase in total abortion patients.
Washington is a “sanctuary state” for abortion, following a directive by Gov. Jay Inslee in 2022 barring police from cooperating with out-of-state investigations regarding abortion. Just this year, Washington also introduced five new pieces of legislation aimed at protecting access to abortion and gender-affirming care.
That legislation includes expanding supply and access to medication abortion, shielding providers and patients in Washington from legal retaliation, increasing privacy around health data and eliminating abortion cost sharing for health plans issued or renewed after January 2024.
Iris Alatorre is the program manager for the Northwest Abortion Access Fund. NWAAF provides financial and travel assistance to people seeking abortions. Between June 2022 to June 2023, NWAAF saw a 61% increase in abortion funding it distributed, a total of $2,181,000, compared to the same period a year prior.
As more people are forced to travel for care because of state abortion bans, many of those patients have to delay care to secure funds, take time off from work, and in some cases, arrange child care, Allatore said.
“That’s an increase overall in the amount of money that is being spent on people accessing abortion care,” they said. “Someone who is maybe in their first trimester of pregnancy, delaying their abortion care and having to wait, maybe until their second trimester of pregnancy, to be able to get the resources together.”
While some patients are able to travel without too much difficulty, Alatorre said, patients who are poor, rural or face bias due to factors like medical racism or gender identity often struggle to access abortions.
Linda McCarthy, CEO of Mt. Baker Planned Parenthood, said some patients travel thousands of miles for abortion care because of bans in their home states. “It’s surreal to think that people have to travel 2,000 miles to come to Bellingham or Mount Vernon, to access a safe, legal abortion,” she said.
The uncertain legality of providing care
(Runtime 00:46)
Clinic staff often find they are also advising patients on life choices, McCarthy said, like where to live and work, because of the impacts that could have on their reproductive care. She gave an example of one patient who was dealing with a possible ectopic pregnancy, which are never viable and can kill the mother. McCarthy said staff advised the patient not to move to Texas for work. “Our providers are like, ‘This is too dangerous for you. We don’t know whether you’ll get the care that you need [in Texas],’” she said.
Alatorre said NWAAF helps people from all walks of life, including parents who are unable to provide for another child, or have pregnancies with fetal abnormalities that make the pregnancy unviable.
“We see a lot of unhoused people needing to access abortion care, people who use drugs,” Alatorre said. “We also, obviously, sometimes see minors. But also like, young, young girls.”
Dr. Mollie Nisen is a Seattle family medicine physician, and an abortion provider who’s seeing more patients traveling out-of-state for abortion.
She says now she’s having to think about what laws are in place where patients are from.
“I’ve never had to be in a position where I’m questioning the legality of what I’m doing as a provider, in a way that is not evidence based,” Niesen said.
Now, she’s needing to consider things like flight schedules when prescribing abortion medications.
Patients often struggle with the financial burden of traveling, and the emotional burden from having to wait longer for care, she said.
Nisen often advises traveling patients on their legal rights, timing when they take abortifacients so they don’t go through treatment in a state where abortion is illegal and provide information about accessing additional care safely, should they need it. For instance, she said, patients need to know that no blood test exists for the abortion drugs mifepristone or misoprostol.
“If a person were to go to an emergency room after a medication abortion, and were to say, ‘I have just had a miscarriage, I need management.’ That, medically, it is not different, and they should be able to seek the care that they need without facing criminalization,’” Nisen said.
Abortion funds struggling to keep up
Since the Dobbs v. Jackson Women’s Health Organization decision, Alatorre said, NWAAF received an outpouring of support from donors including some state and local governments. Other abortion funds, in states like Arizona and Utah, often don’t have the same level of support.
“They have a much smaller budget to work with, and they’re having to spend that budget way quicker,” she said. “So, that means that people who are needing abortion care and calling their local funds to get care sometimes are turned away, because the fund has spent all of their money for that month.”
NWAAF primarily serves Washington, Alaska, Idaho and Oregon, but has helped people seeking abortions from 42 different states.
Last year, NWAAF served 762 people from Washington, 430 from Idaho, 404 from Oregon, 147 from Texas and 103 from Alaska.
Alatorre said NWAAF staff are dealing with new challenges because demand for assistance more than doubled in the last year.
“We have had to scale up so quickly, so fast, it’s hard to keep up,” she said. “We are understaffed and therefore the folks who are doing this work, we are burning out.”
Though the organization has been met with an influx of both funding and volunteers, training those volunteers is a lengthy process.
Volunteers are asked to commit a minimum of two years because of the time and energy it takes to train them.
Different people will also be able and willing to take on different levels of legal risk, she said. Laws like Idaho’s so-called “abortion trafficking” law criminalize anyone who helps a minor obtain an abortion without parental consent.
“It is such a labor-intensive process for the folks who are doing the vetting and onboarding and training. It takes a while for us to do it the way we would like to do it,” they said. “That slows down the pace at which we can bring more people on.”
Karl Eastlund, CEO of Planned Parenthood of Greater Washington and North Idaho, said the Pullman, Walla Walla and Kennewick clinics have seen the biggest increase in patients due to a Meridian clinic no longer offering abortion.
“The big shift was there was an abortion clinic in Meridian, outside of Boise,” he said. “Those are the patients that are 100% displaced.”
Across the board, Eastlund said, clinics have seen between roughly 70 to 100 new visits a month, accounting for somewhere between 20-30% increases, depending on the clinic.
Wait times have not significantly increased in Washington clinics, Eastlund said, though some clinics have had to expand hours, and prioritize abortion over other services on some clinic days.
“I think it was what many of us had feared was coming. And so we were already starting to get ready for an anticipated surge from Idaho,” he said.
In 2022, the Pullman Planned Parenthood clinic reported seeing its Idaho-based patients jump from 62% in June to 78% in July, despite Idaho’s abortion ban only taking effect August 25, according to Cantwell’s office.
Even some Washington residents are traveling across the state to get quicker access to reproductive care, McCarthy said.
“We’re seeing people from other areas in Washington state because some of the other border clinics are busier with people coming that are closer,” McCarthy said.
Some patients — even Washington residents — are seeking long-acting reversible contraception, such as IUDs because of the Dobbs decision, she said.
“They just want to protect themselves and get that device implanted or inserted now, so that it’s available to them for a long term, and you don’t have to worry about what might come,” McCarthy said.
The closure of Idaho clinics have also limited access to non-abortion OB-GYN care for Idaho patients.
That impact isn’t just at clinics to provide abortion. Two Idaho hospitals, Bonner General Health in Sandpoint and Valor Health Hospital in Emmet, closed their labor and delivery units this spring, citing challenges recruiting skilled doctors and nurses. Bonner General specifically cited Idaho’s political climate as a challenge in OB-GYN recruitment.
“Highly respected, talented physicians are leaving,” the March press release stated. “Recruiting replacements will be extraordinarily difficult. In addition, the Idaho Legislature continues to introduce and pass bills that criminalize physicians for medical care nationally recognized as the standard of care. Consequences for Idaho Physicians providing the standard of care may include civil litigation and criminal prosecution, leading to jail time or fines.
Changing medical landscape
A survey this spring of Idaho doctors who work in maternal fetal health asked physicians if they were considering relocating. Of respondents, 48 said yes, 42 no, and 27 said maybe. 73 out of 75 of the doctors said the state’s abortion laws contributed to their reason for leaving.
Dr. Loren Colson is a full-spectrum family medicine doctor in Boise who provides outpatient, inpatient and obstetrics care. He said he’s considered leaving, though hadn’t made the decision to do so yet.
“There’s a point where just ethically, I cannot continue providing care if there are too many restrictions on the way that I provide that care, because I can’t live up to my ethical medical standard,” Colson said.
Colson said he’s worried if further restrictions are passed on contraception, it might be impossible to meet those standards. The state’s tightening restrictions have also changed his approach to care for patients who could get pregnant.
“We always offer emergency contraception, and told our patients that there’s over-the-counter emergency contraception too. But now, we just try and identify folks that are of reproductive potential, and then just prescribe it to them and tell them, ‘It’s probably best just to have this on hand.’”
Idaho’s Defense of Life Act leaves doctors open to prosecution for assisting in an abortion. This has also left doctors uncertain of whether they can safely or legally talk to their patients about resources outside the state.
A March letter from Idaho Attorney General Raul Labrador stated that Idaho medical providers referring patients across state lines for abortion or prescribing abortion pills for patients to pick up in another state would be considered assisting in an abortion.
Labrador later withdrew the letter after a lawsuit was filed by Planned Parenthood, and suggested it was not intended as a guiding document. However, it’s continued to have a chilling effect, Colson said.
“It’s really hard,” he said. “People come to us expecting to be able to have a frank conversation with their physician and get whatever care that they need. And that is something that we can’t provide them with now.”
Training Idaho’s medical workforce
Abortion restrictions are making it harder for states with bans to recruit new medical providers and to train the medical workforce in those states. A residency program in Boise was forced to stop abortion training through a Planned Parenthood clinic.
Those residents now must to travel to Spokane, or farther, without support from their program.
A survey by the Association of American Medical Colleges found applications for U.S. senior doctor of medicine OB-GYN residencies decreased by 10.3% in 2023 in states with complete bans, with a 5.2% decrease across the U.S. The same survey found a drop in applicants seeking residencies in other areas likely to be impacted by the bans, such as -21.4% for emergency medicine and -3% for family medicine.
Colson said medical residents he knows are troubled by not being able to access some kinds of training.
“I think for medical students and for residents, we know that this is a big issue for them,” he said. “Even if they’re not interested in necessarily training in abortion, I think the idea of practicing in states that are limiting medical care is very concerning.”
Idaho has continually struggled to provide adequate health care for its residents. A 2022 report by Idaho Business for Education found the state had around 9,000 unfilled health care positions.
Dr. Sarah Prager is a professor of obstetrics and gynecology at the University of Washington. She said some students are reconsidering plans to practice in states with strict abortion bans.
“Students who potentially always planned to go back to their home state of Idaho or Wyoming or Alaska, or farther afield, who now are deciding if they can be the kind of provider that they wanted to be in their home state,” Prager said.
Colson said abortion bans affect providers across the state, even if they don’t specialize in obstetrics, gynecology or maternal health.
“There’s physicians out there saying, ‘This doesn’t affect me, because I don’t provide abortions.’ But it does affect you, because it affects who you can refer to,” he said. “It affects whether doctors want to stay in the state, it worsens our already large health provider shortage that we have in Idaho.”
Editor’s note: This story was updated to correct a statement regarding the Meridian Planned Parenthood clinic. The clinic is open, but does not provide abortion services.